19A125
Audit on osteoporosis assessment and management in patients with chronic obstructive pulmonary disease (COPD)
Author(s)
Sonia Sundanum, Katherine Finan
Department(s)/Institutions
Department of respiratory medicine, Sligo University Hospital, Saolta University Health Care Group
Introduction
COPD is a chornic airway inflammatory disease associated with multiple co-morbidities including osteoporosis. Osteoporotic fractures have dramatic impacts on quality of life and even respiratory fucntion in patients with COPD.
COPD associated osteporosis is however hugely under-recognised and under treated.
Various risk factors of osteoporosis in COPD patients, including older age, low body mass index, physical inactivity, smoking, cortisosteroid use and vitamin D deficiency have been described.
Aims/Background
We aimed to determine whether patients attending the respiratory department with a diagnosis of COPD were screened for osteoporosis and getting the appropriate treatment.
Method
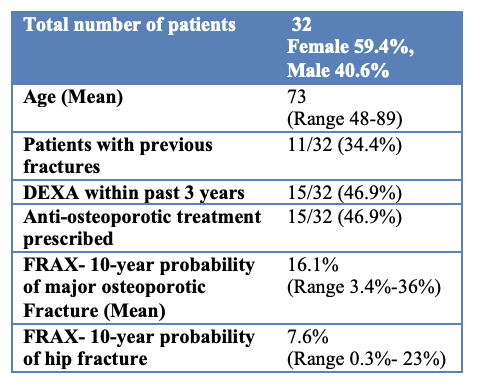
32 patients attending the respiratory outpatient department with a diagnosis of COPD were included.
We evaluated the following: their bone mineral density (BMD) using bone densitometry scan (DEXA) in the past 3 years, their 10-year probability of bone fracture risk was calculated using the Fracture Risk Assessment Tool (FRAX), the use of anti-osteoporotic treatment for these patients.
Results
26/32 patients were over 65 years old and 15 of these were on adequate anti-osteoporotic treatment.
Out of 11 patients with previous fractures; 3 were not recorded to being prescribed for bone protection and 3 did not have a DEXA scan within the previous 3 years.
Out of the 6 patients with a diagnosis of osteoporosis based on their BMD; 5 were adequately prescribed with bone protection.
The commonest site for fracture was vertebral (6/11); other fracture sites included wrist, pubic ramus, humerus, rib, and finger.
Conclusions
Recent studies would advise that any symptomatic COPD patient over the age of 50 years old should be screened for potential indication of pharmacological treatment.
FRAX underestimates the COPD-associated fracture risk and additional risk factors such as reduced physical activity; severely impaired lung function and height loss should be included in risk stratification.
Patients at potential risk should then be examined for BMD by DXA.
Prevalent vertebral fractures and systemic corticosteroid therapy are a strong indication of medical treatment.
Until a specific treatment guideline for COPD-associated osteoporosis is proposed, individuals with COPD should be screened, early diagnosis should be made and treatment measures put in place to prevent future fracture risk.
Figure