18A165
ERASMUS syndrome presents with Scleroderma renal crisis and Subarachnoid hemorrhage
Author(s)
Tariq S, Sebastian A, Anjum A, Ng WL, Adeeb F, Devlin J, Fraser A.
Department(s)/Institutions
Rheumatology Department, University Hospital Limerick
Introduction
Erasmus syndrome is the rare association of Systemic Sclerosis (SSc) with silica exposure, cigarette smoking and Interstitial lung disease resulting in a severe disease phenotype. Scleroderma Renal Crisis (SRC) is a rheumatological emergency and a severe complication of scleroderma which can occur up to 10% of the SSc patients. SRC presents with abrupt onset of moderate to marked hypertension, acute renal failure, thrombocytopenia and hemolytic anemia. Blood pressure control with angiotensin-converting enzyme (ACE) inhibitors is the cornerstone of treatment.
Aims/Background
Case Report
Method
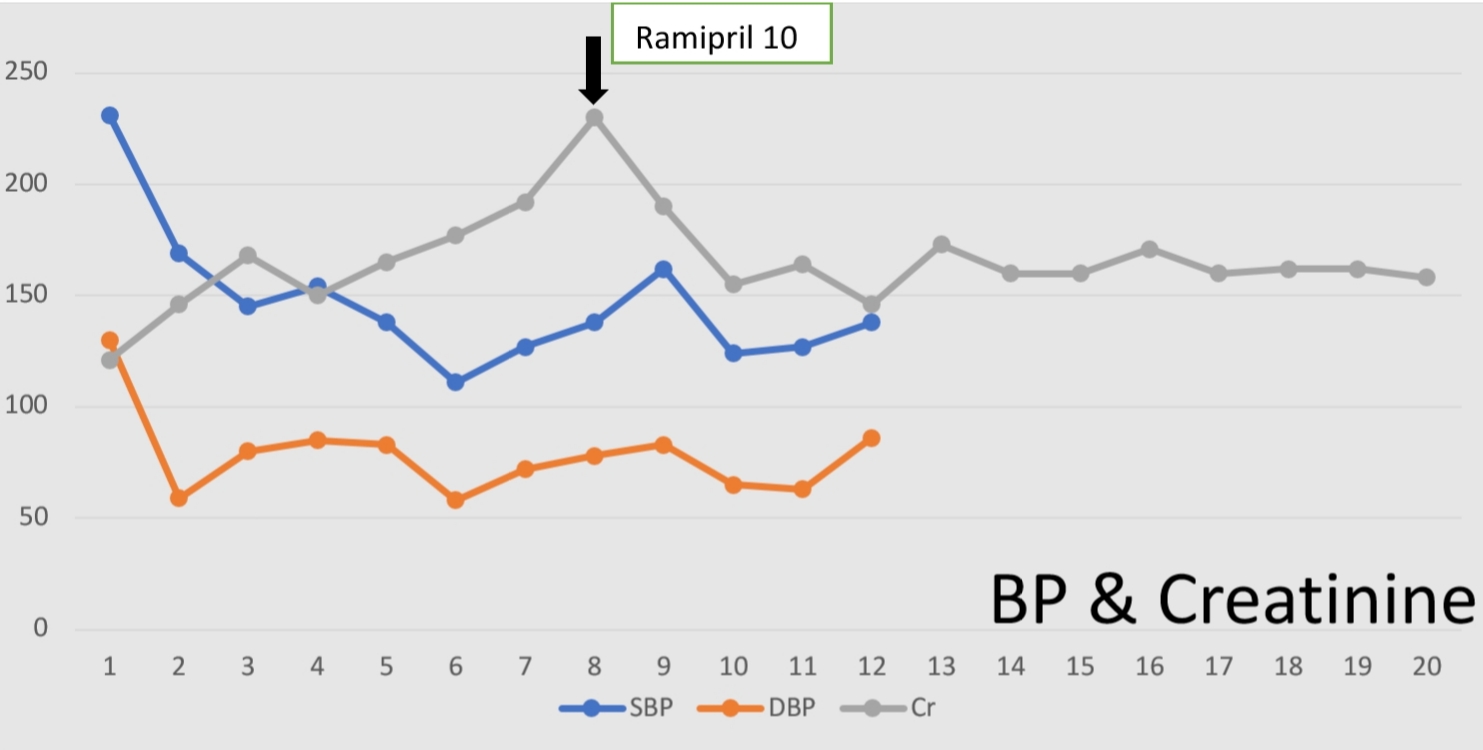
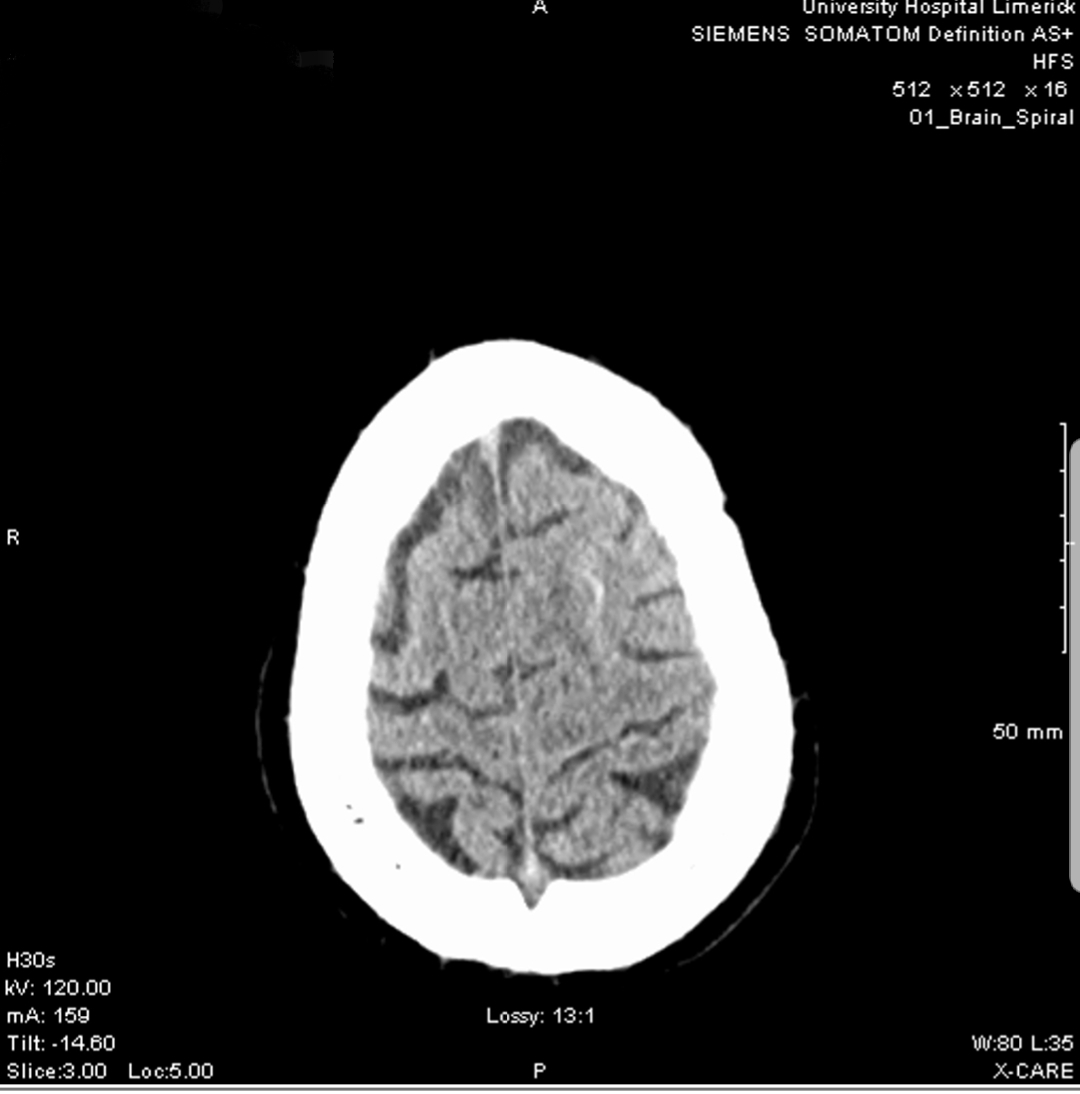
A 50 years old man presented with five days history of severe headache and photophobia. Clinical examination revealed blood pressure of 231/130mmHg and marked neck stiffness. He had a recent diagnose of Erasmus Syndrome and was taking Oral glucocorticoids, Nifedipine and Mycophenolate Mofetil. His serology showed positive ANA (400) and anti Ro antibodies. However, Scl70 and anti-centromere antibodies were negative. His initial presentation also revealed acute kidney injury (AKI), thrombocytopenia, mild anemia and normal CT brain. Later that day he had two episodes of witnessed tonic-clonic seizures for which he required intubation and transfer to Intensive Care Unit (ICU). Urgent repeat CT brain revealed bilateral subarachnoid hemorrhage (Image-1) and the CT cerebral angiogram raised the possibility of middle cerebral artery vasculitis. MRI/MRA brain confirmed he had bilateral subarachnoid hemorrhage. Neurosurgeons advised no surgical intervention required. He was started on IV methylprednisolone and IV broad spectrum antibiotics in the ICU. He was later reviewed by the rheumatologist and promptly diagnosed with SRC and commenced on Ramipril (ACE inhibitor). His IV steroids and antibiotics were discontinued. His blood pressure was controlled with Ramipril and Labetalol while he was under the close surveillance of his renal function (Image-2).
Results
This gentleman recovered from SRC with ACE inhibitor treatment but suffered a chronic kidney injury (Creatinine now averages 150, eGFR 40. In the follow up rheumatology clinic he was commenced on Rituximab (anti CD-20 antibody) as an adjuvant therapy.
Conclusions
Scleroderma renal crisis is a medical emergency and prompt diagnosis and early treatment with ACE inhibitor has a promising outcome.
Figure
Figure